Bronchial Asthma
Definition
A chronic inflammtory condition of the bronchi and bronchioles
Causes narrowing of the air passages
Obstructs air flow
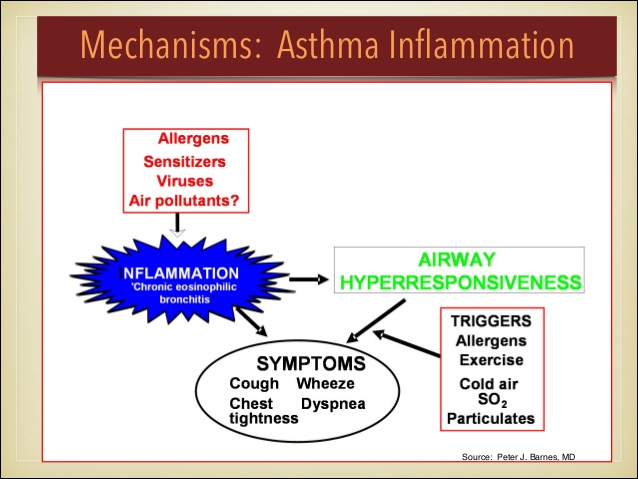
Causes
Allergens, sensitizers, viruses, air pollutants, Cold air, SO2, exercise
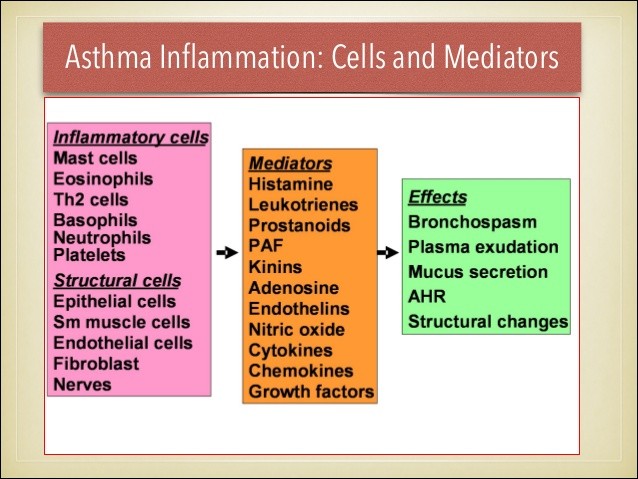
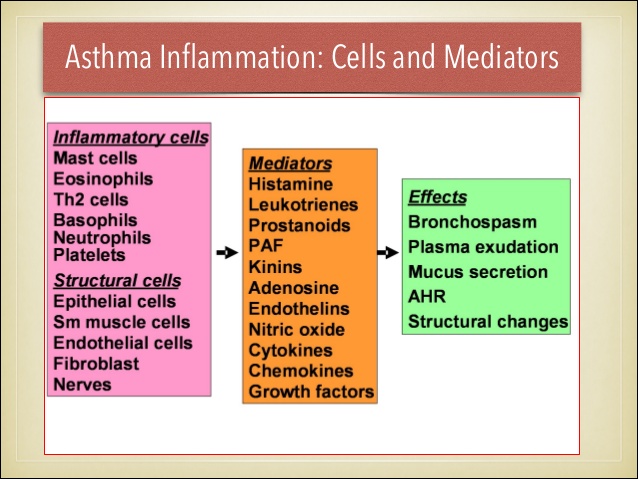
Pathophysiology
Triggering factors cause inflammation (Chronic eosinophilic bronchitis)
Air passing through narrow passages causes whisling sound
inflammotary cells appear in the mucosa
Mucus produced
When the alphaadrenergic receptors are stimulated, bronchoconstriction occurs;
When the beta2-adrenergic receptors are stimulated, bronchodilation
(Betablocers used in hypertension to be avoided in patients of B.Asthma
Clinical Features
Cough
Dyspnoea
Wheezing
Usually at nights
Accessory muscles act
Expiratory wheeze more than inspiratory wheeze
Tachycardia
Seasonal exacerbations +
Lab Tests
Done for recurrent asthma to identify substances that precipitate the symptoms
Complications
Status asthmaticus
Respiratory failure
Pneumonia
Atelectasis
Hypoxemia
Dehydration
Medical Management
Pharmacologic Therapy
Prevention
Do tests to identify the allergen
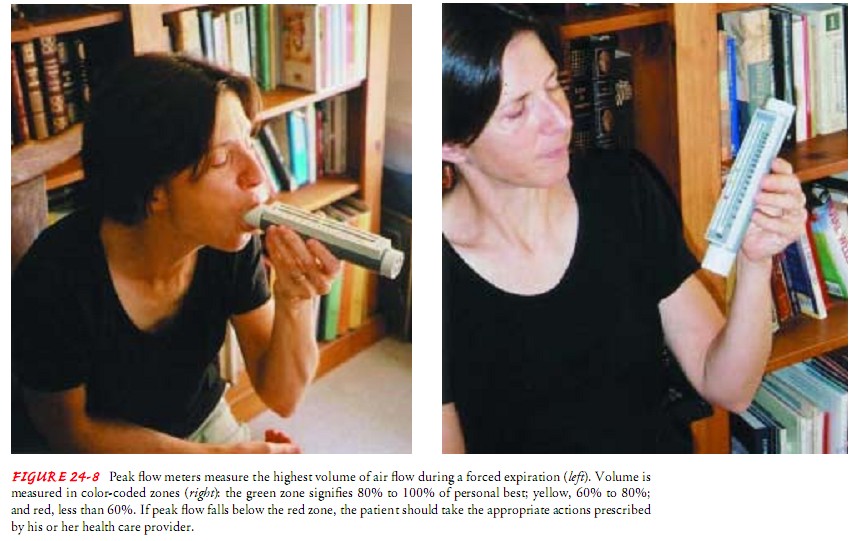
Provide the patient with peak flow meter for monitoring the severity
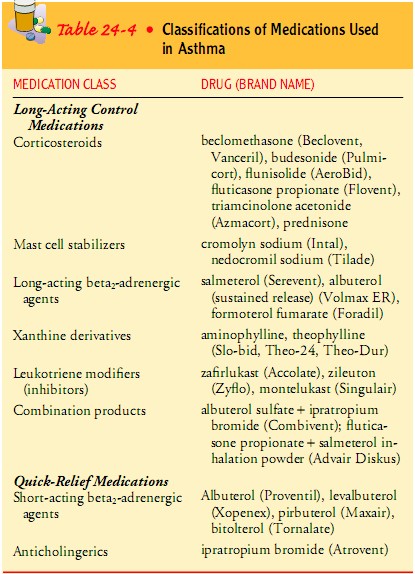
Pharmacologic Therapy
Long acting drugs
Short and quick acting drugs
Choice of treatment is MDI - Spacer device -
Drugs given Systemically for moderate to severe attack
Cromolyn sodium and nedocromil commonly used in children - for prevention also - contraindicated in acute asthma exacerbations
Bronchodilators must be combined with steroids because asthma is a chronic inflammatory condition
Systemic corticosteroids needed when inhaled medications fail.
O2 whenever needed
Nebulization with broncho dilators and steroids needed at times
Commonly used drugs : Deriphylline, Theophylline, Salbutamol, Terbutaline, Budecort, Prednisolone, Dexamethasone, Hydrocortisone, Oxygen
592
Assessment
HEALTH HISTORY AND
CLINICAL MANIFESTATIONS
A comprehensive allergy history and a thorough physical exami-
nation provide useful data for the diagnosis and management of
patients with allergic disorders. An assessment form is useful for
obtaining and organizing this information (Chart 53-1).
The degree of dif?culty and discomfort experienced by the pa-
tient because of allergic symptoms and the degree of improve-
ment in those symptoms with and without treatment are assessed
and documented. The relationship of symptoms to exposure to
possible allergens is noted.
Diagnostic Evaluation
Diagnostic evaluation of the patient with allergic disorders com-
monly includes blood tests, smears of body secretions, skin tests,
and the radioallergosorbent test (RAST). Results of laboratory
blood studies provide supportive data for various diagnostic pos-
sibilities; however, they are not the major criteria for the diagno-
sis of allergic disease.
COMPLETE BLOOD COUNT
WITH DIFFERENTIAL
The white blood cell (WBC) count is usually normal except with
infection. Eosinophils, granular leukocytes, normally make up
1% to 3% of the total number of WBCs. A level between 5% and
15% is nonspeci?c but does suggest allergic reaction. Higher levels
are considered moderate and severe. In moderate eosinophilia,
15% to 40% of blood leukocytes as eosinophils are found in
patients with allergic disorders as well as in patients with malig-
nancy, immunode?ciencies, parasitic infections, and congenital
heart disease, and those receiving peritoneal dialysis. In severe
eosinophilia, 50% to 90% of blood leukocytes as eosinophils are
found in the idiopathic hypereosinophilic syndrome.
EOSINOPHIL COUNT
An actual count of eosinophils may be obtained from blood sam-
ples or smears of secretions. A total eosinophil count can be ob-
tained from a blood sample by using special diluting ?uids that
hemolyze erythrocytes and stain the eosinophils. During symp-
tomatic episodes, smears obtained from nasal secretions, con-
junctival secretions, and sputum of atopic patients usually reveal
eosinophils, indicative of an active allergic response.
TOTAL SERUM
IMMUNOGLOBULIN E LEVELS
High total serum IgE levels support the diagnosis of atopic dis-
ease. A normal IgE level, however, does not exclude the diagno-
sis of an allergic disorder. IgE levels are not as sensitive as the
paper radioimmunosorbent test (PRIST) and the enzyme-linked
immunosorbent assay (ELISA). Indications for determining IgE
levels include the following:
• Evaluation of immunode?ciency
• Evaluation of drug reactions
• Initial laboratory screening for allergic bronchopulmonary
aspergillosis
• Evaluation of allergy among children with bronchiolitis
• Differentiation of atopic and nonatopic eczema
• Differentiation of atopic and nonatopic asthma and rhinitis
SKIN TESTS
Skin testing entails the intradermal injection or super?cial appli-
cation (epicutaneous) of solutions at several sites. Depending on
the suspected cause of allergic signs and symptoms, several dif-
ferent solutions may be applied at several separate sites. These so-
lutions contain individual antigens representing an assortment of
allergens, including pollen, most likely to be implicated in the pa-
tient’s disease. Positive reactions (wheal and ?are) are clinically
signi?cant when correlated with the history, physical ?ndings,
and results of other laboratory tests.
The results of skin tests complement the data obtained from
the history. They indicate which of several antigens are most
likely to provoke symptoms and provide some clue to the inten-
sity of the patient’s sensitization. The dosage of the antigen (al-
lergen) injected is also important. Most patients are hypersensitive
to more than one pollen. Under testing conditions, they may not tion at the end of a wheal) with associated erythema is considered
react (although they usually do) to the speci?c pollens that induce indicative of sensitivity to the corresponding antigen.
their attacks. There may be false-negative results due to improper tech-
In cases of doubt about the validity of the skin tests, a RAST nique, outdated allergen solutions, and prior use of medications
or a provocative challenge test may be performed. If a skin test is that suppress skin reactivity. Corticosteroids and antihista-
ndicated, there is a reasonable suspicion that a speci?c allergen mines, including allergy medications, suppress skin test reactiv-
s producing symptoms in an allergic patient. Several precau- ity and are usually withheld 48 to 96 hours before testing,
tionary steps, however, must be observed before skin testing with depending on the duration of their activity. False-positive skin
allergens: tests may result from improper preparation or administration of
allergen solutions.
• Testing is not performed during periods of bronchospasm.
Interpretation of positive or negative skin tests must be based
• Epicutaneous tests (scratch or prick tests) are performed be-
on the history, physical examination, and other laboratory test
fore other testing methods in an effort to minimize the risk
of systemic reaction.
• Emergency equipment must be readily available to treat
anaphylaxis.
Types of Skin Tests
The methods of skin testing include prick skin tests, scratch tests,
and intradermal skin testing (Fig. 53-3). After prick or scratch
tests, intradermal skin testing is performed with allergens that did
not elicit positive reactions. Because a larger antigen challenge is
being used, local or systemic reactions could occur if the same
antigens that produced positive skin or scratch reactions are used.
The back is the most suitable area of the body for skin testing be-
cause it permits the performance of many tests. The multitest ap-
plicator is a commercially available device with multiple test
heads that allows simultaneous administration of antigens by
multiple punctures at different sites.
FIGURE 53-3 Intradermal testing. A 0.5-mL or 1-mL sterile syringe with
Interpretation of Skin Test Results a 26/27 gauge intradermal needle is used to inject 0.02 to 0.03 mL of intra-
dermal allergen. The needle is inserted with the bevel facing upward and the
Familiarity with and consistent use of a grading system are es-
syringe parallel to the skin. The skin is penetrated super?cially, and a small
sential. The grading system used should be identi?ed on a skin
amount of the allergen solution is injected to create a bleb (raised area) ap-
test sheet for later interpretation. A positive reaction, evidenced
proximately 5 mm in diameter. A separate sterile syringe and needle are used
by the appearance of an urticarial wheal (round, reddened skin for each injection. From Taylor, C., Lillis C., & LeMone, P. (2001). Fun-
elevation) (Fig. 53-4), localized erythema (diffuse redness) in the damentals of nursing: The art and science of nursing care (4th ed.). Philadel-
area of inoculation or contact, or pseudopodia (irregular projec- phia; Lippincott Williams & Wilkins.
results. The following guidelines are used for the interpretation tions. The major disadvantages include the limited allergen se-
of skin test results: lection, reduced sensitivity compared with intradermal skin tests,
lack of immediate results, and cost.
• Skin tests are more reliable for diagnosing atopic sensitivity
in patients with allergic rhinoconjunctivitis than in patients
with asthma. Allergic Disorders
• Positive skin tests correlate highly with food allergy.
• The use of skin tests to diagnose immediate hypersensitivity There are two types of IgE-mediated allergic reactions: atopic
to medications is limited because metabolites of medica- and nonatopic disorders. While the underlying immunologic re-
tions, not the medications themselves, are usually responsi- actions of the two types of disorders are the same, predisposing
ble for causing hypersensitivity. factors and manifestations are different. The atopic disorders are
characterized by a hereditary predisposition and production of a
local reaction to IgE antibodies produced in response to com-
PROVOCATIVE TESTING
mon environmental allergens (Kay, 2001a). The nonatopic dis-
Provocative testing involves the direct administration of the sus- orders lack the genetic component and organ specificity of the
pected allergen to the sensitive tissue, such as the conjunctiva, atopic disorders (Porth, 2002). Examples of atopic disorders are
nasal or bronchial mucosa, or gastrointestinal tract (by ingestion allergic rhinitis, allergic asthma, and atopic dermatitis (Kay,
of the allergen) with observation of target organ response. This 2001a).
type of testing is helpful in identifying clinically signi?cant aller- A type I hypersensitivity response results in atopic (allergic) dis-
gens in patients with a large number of positive tests. Major dis- eases, which affect 10% to 20% of the U.S. population. Genetic
advantages of this type of testing are the limitation of one antigen factors play a role in susceptibility to these diseases. Disorders char-
per session and the risk of producing severe symptoms, particu- acterized as atopic include anaphylaxis, allergic rhinoconjunctivi-
larly bronchospasm, in patients with asthma. tis, atopic dermatitis, urticaria and angioedema, gastrointestinal
allergy, and asthma. Latex allergy may be a type I or type IV hyper-
sensitivity reaction, although true latex allergy is considered to be
RADIOALLERGOSORBENT TEST
a type I hypersensitivity reaction (Brehler & Kütting, 2001). Latex
RAST is a radioimmunoassay that measures allergen-speci?c IgE. allergy is discussed later in this chapter. Contact dermatitis is con-
A sample of the patient’s serum is exposed to a variety of sus- sidered a type IV hypersensitivity reaction.
pected allergen particle complexes. If antibodies are present, they
will combine with radiolabeled allergens. After the serum is cen-
ANAPHYLAXIS
trifuged, radioimmunoassay detects the allergen-speci?c IgE an-
tibody. Test results are then compared with control values. In Anaphylaxis is a clinical response to an immediate (type I hyper-
addition to detecting an allergen, RAST indicates the quantity of sensitivity) immunologic reaction between a speci?c antigen and
allergen necessary to evoke an allergic reaction. Values are re- an antibody. The reaction results from IgE antibody. An ana-
ported on a scale from 0 to 5. Values of 2+ or greater are consid- phylactic reaction can be triggered by exposure to an antigen
ered signi?cant. The major advantages of RAST over other tests through inhalation, injection, ingestion, or skin contact. It is a se-
include decreased risk of systemic reaction, stability of antigens, vere, life-threatening allergic reaction. It is estimated that 3.3 to
and lack of dependence on skin reactivity modi?ed by medica- 43 million persons in the United States (1.24% to 16.8% of the